 Fresh from planning new inpatient units through to design development my recent experience of designing code compliant patient toilets for 150 newly constructed rooms has given me insight on a few key planning considerations in the future will save me time and re-work (and possibly some sanity).
Fresh from planning new inpatient units through to design development my recent experience of designing code compliant patient toilets for 150 newly constructed rooms has given me insight on a few key planning considerations in the future will save me time and re-work (and possibly some sanity).
First and foremost, I cannot stress enough the importance of studying the applicable codes and understanding the impact they will have on the patient room design early in the planning process. Here are a few more:
- Gain an early understanding of the projects goals and objectives around handicap accessibility needs. A few examples:
– Space program must include a minimum of 10% of all room types shall meet code but clients may ask for more.
– Identify construction constraints such as back-to-back toilets for shared chases, no fixtures to be placed on exterior walls; door size and type requirements
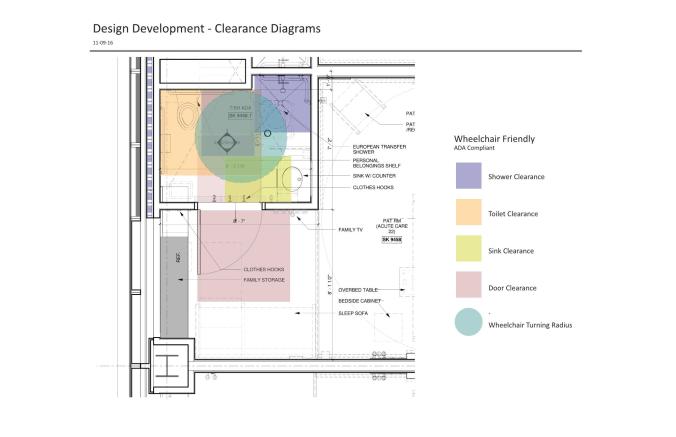
– Is the planning/design team considering creative space-saving ideas, such as sliding glass doors or an open “European” shower concept that allows for greater mobility in the toilet room?
- Reach out to the accessibility code consultant early and often and give them the opportunity to weigh in on design options and considerations. Having a collaborative relationship provides the best outcomes
- Plan in enough time for the design process. Don’t underestimate the hours it will take to review code requirements and their positive and negative impacts on the proposed design.
- Research all the applicable accessibility codes for your project. They vary from state to state. Projects in Massachusetts need to meet both federal ADA Standards and MAAB (Massachusetts Architectural Access Board) 521 CMR.


- Know that it is not possible to have only 1 type of handicap accessible patient toilet room on a Massachusetts project. 521 CMR states that of the 10% handicap accessible rooms, 5% need to meet “Transfer Type” shower, and 5% need to meet “Standard Roll-In Type” shower.
- Identify specific requirements between applicable codes. There are different requirements between ADA Standards and 521 CMR and we have to design to the most stringent code. If a discrepancy doesn’t yield a more stringent requirement, then both codes need to be met.
– For example: ADA Standards requires the 36″x48” clear floor space for transfer type shower to be adjacent to the shower and aligned with the shower control wall (#608.2.1). However, MAAB 521 CMR requires the 36″x48” clear floor space to on center of the shower enclosure (#42.7.2 [b]). Because neither one is more stringent, a 6” offset is required at the control wall in order to maintain the 24” clearance from the enclosure’s center line, resulting in an overall clear floor space of 36”x54”.
- EUROPEAN SHOWERS – Well-designed European showers (open shower concept with 2 walls instead of 3) are a great idea for gaining more space in a toilet room where space is a constraint and when showers are used infrequently but still required. If you are planning on European showers, please be aware that a variance may be required in order to achieve a code compliant intended design.






